SOAP 2.0 | Daily Notes
- 05 Apr 2024
- 2 Minutes to read
- Print
- DarkLight
- PDF
SOAP 2.0 | Daily Notes
- Updated on 05 Apr 2024
- 2 Minutes to read
- Print
- DarkLight
- PDF
Article Summary
Share feedback
Thanks for sharing your feedback!
Overview
WebPT's Daily Notes feature is your go-to tool for efficient and comprehensive patient documentation. When it's time to jot down another note on your patient's progress, simply navigate to their chart, where the SOAP 2.0 Patient Records Page will automatically load if documentation has been initiated. From there, selecting Create Daily Note gets you started. Whether it's a Daily Note or another type like a Case Note, just tap the menu button to access the options.
Each section in the note displays a Last updated DOS tag from the previous entry, ensuring you're working with the latest information. Editing or adding to any subsection is a breeze—just click and make your adjustments. Plus, with SOAP 2.0's Integrated Flowsheets, activities and interventions seamlessly carry forward, streamlining your workflow.
Remember, in the Patient Presentation section, updating or adding to the note is a must for completeness. Throughout the note, pertinent sections like Diagnosis, Problems & Goals remain in Read-mode, saving space while keeping you informed. And don't forget to finalize or adjust charges before signing off.
With WebPT's Daily Notes, staying organized and up-to-date has never been easier. Sign off confidently, knowing your documentation is thorough and accurate.
Click the arrow or colorblock below to discover more.
Add a Daily Note
SOAP 2.0 | Add a Daily Note
When it’s time to document another note on your patient, go to the patient’s chart. When documentation for the patient has been started in SOAP 2.0, the SOAP 2.0 Patient Records Page automatically loads.
Select Create Daily Note. Remember, if you want to add a different type of note, such as a Case Note, select the (...) menu button.
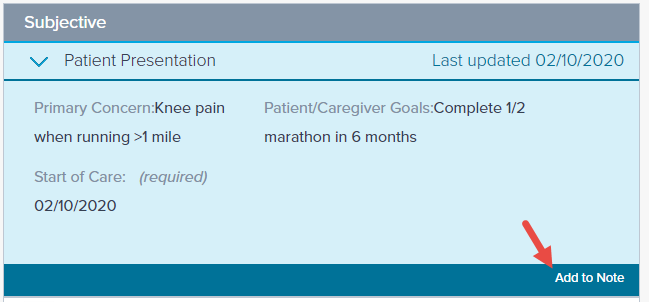
Each section with information entered will have a ‘Last updated’ date of service tag from the previous note where the information was updated.

Click on the subsection to review/edit the information as necessary, then edit or Add to Note to carry forward the information as is.
Document activities and interventions with SOAP 2.0's Integrated Flowsheets. Flowsheet documentation carries forward from one note to the next.
You must update or Add to Note in the Patient Presentation section.
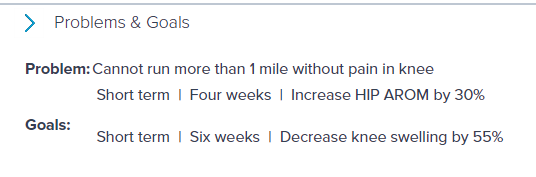
Subsections with pertinent information (like Diagnosis, Problems & Goals, etc.) appear in Read-mode throughout the note. This allows you to quickly determine whether they need to be updated without taking up extra space.
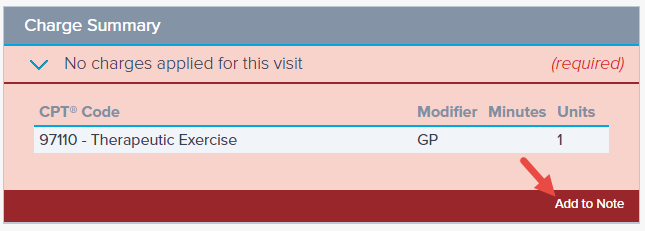
You must click Add to Note or edit the charges to successfully sign the note. Discover more about the carry forward functionality of the Charge Summary section.
When you’ve finished documenting, Sign the note.






Was this article helpful?